MentalHealthCE Login


| Login | ||

Healthcare Training Institute - Quality Education since 1979
CE for Psychologist, Social Worker, Counselor, & MFT!!

Section 12
Models of Borderline Personality
Question
12 | Test
| Table of Contents
Confusion over the use of the term borderline as a psychiatric diagnosis
is almost axiomatic, but this has neither hindered the term's rapid acceptance
and wide application, nor led to a systematic delineation of the syndrome. The
literature on the borderline patient is growing rapidly, but so far not a single
investigation has been undertaken to reveal the extent to which clinicians agree
on the definition of borderline or achieve consensus when making this diagnosis.
The question of whether "borderline" merits a place in psychopathologic
nosology can hardly be debated intelligently before we resolve these basic points.
Before beginning this process, however, it is necessary to review the several
models of psychopathology that can be applied to the concept of the borderline
patient. These models have remarkably different implications.
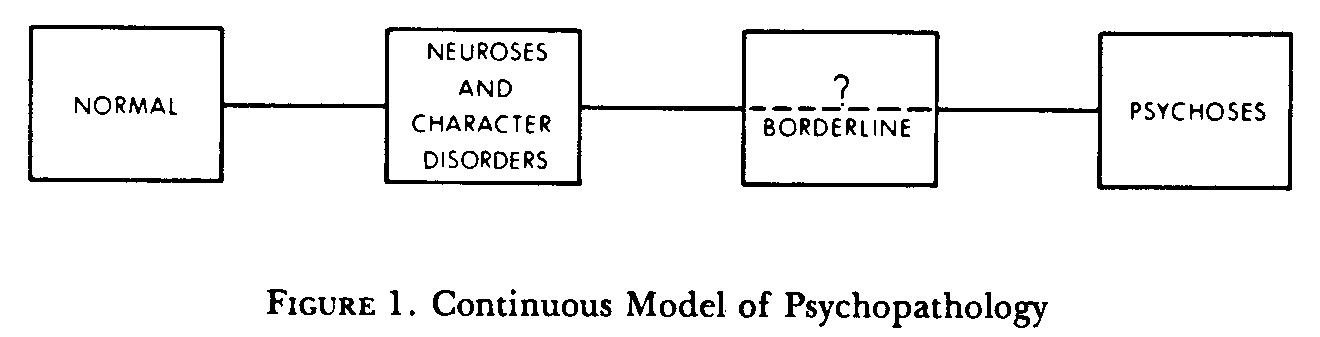
The most common concept of borderline is based on a continuum or dimensional model of psychopathology, as is represented in Figure 1. In simplest terms, behavior or psychological functioning is viewed as ranging from normal to severely psychotic. Menninger has used this model exclusively in classifying mental disorders in his book The Vital Balance (Menninger, Mayman, and Pruyser, 1963). Neuroses and character disorder are placed toward the normal end of this continuum. Borderline refers to a disorder with greater severity than neurosis and character disorder but less severity than psychosis. This concept is used by Grinker, Werbie, and Drye (1968). Their four subgroups can be considered as defining subsections on a segment of this continuum, with their Group I on the border with psychoses and Group IV on the border with neuroses.
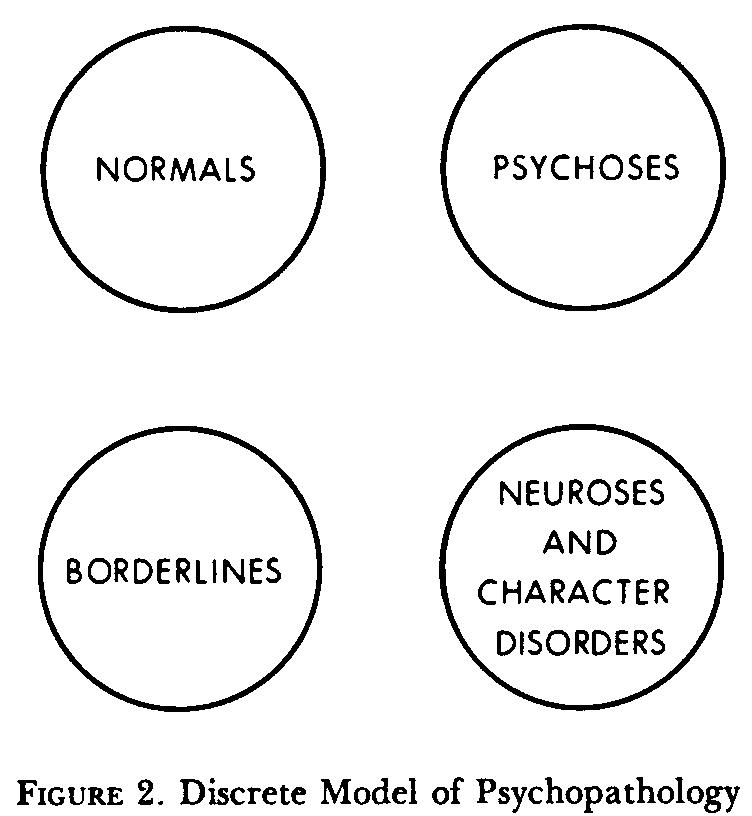
A second model-the typological model-suggests that psychopathology can best be organized into discrete groups not representing a continuum or having any other specific relation to each other (see Figure 2). In this model, nosologic groups are delineated from each other and from normals on the basis of a supposedly qualitative unique characteristic feature. Any pathologic manifestation could range from mild to marked within the group, but the presence of distinguishing features rather than their severity is critical to diagnosis. This model does not imply that no similar psychopathologic features are to be found between groups (e.g., anxiety is almost ubiquitous across diagnostic classes), only that distinguishing features identify patients as belonging to a discrete class.
The theoretical implications of these two concepts are quite different. The first model encourages a search for points on the continuum which can usefully be defined and distinguished from other points. One assumes there will be confusing cases at the interface between any two defined points, and that locating such a boundary case in either group would not be entirely misleading. In contrast, a typologic or discontinuous model of psychopathology does not allow for the intermediate case, and hence the implications are more drastic. An incorrect classification would be entirely misleading, rather than simply underestimating or overestimating the severity of psychopathology. There could be confusing cases, however, either because the disease is only partially manifest or because the patient was simultaneously afflicted with two illnesses.
Considerable evidence has now emerged suggesting some discrete classes of psychopathology. Genetic studies (adoptive, cross-fostering, and family-tree) document that manic-depressive and schizophrenic illness are discrete, and this distinction is supported by differential psychopharmacologic responsivity. On the other hand, if one looks at these two illnesses from a descriptive or an egopsychologic point of view, phenomenologic and ontogenetic observations can be readily conceptualized on a continuum. The concept of schizophrenia spectrum (Kety et al., 1968), derived from genetic investigations, lends support to a continuous model of psychopathology.
In the continuum model the question is whether borderline is a useful segment to delineate. There is no question about the existence of a borderline as there is a border between any two sequential points. The question is pragmatic: Does defining the characteristics of the border provide useful information in terms of etiology, course, or treatment? Is assigning a borderline diagnosis more helpful than diagnosing these patients as either neurotic or psychotic, or relegating them to an uncertain diagnostic status?
If we use a discontinuous model, on the other hand, then we must prove that such a group exists. Nosology implies a capacity to generalize from group membership. Assignment to an invalid class would be totally misleading.
The use of borderline as a diagnosis if this category is inadequately defined has different implications in the two models discussed. On a continuum model, a poorly defined point would lead to sloppy diagnostic practices reducing the usefulness of the better-defined surrounding points. In the discontinuous model a poorly defined entity would have little chance of being validated, hence its existence as well as usefulness would be in question.
A third model for classification combines the properties of the continuum and typological approaches. Such a combined or mixed model provides the means for integrating the presently available conflicting data relevant to psychiatric nosology. A mixed model can define two levels-a continuous and a discrete level- allowing one to conceptualize disordered ego functioning and character development along a severity continuum but hypothesizing that at certain segments of this continuum psychopathologic manifestations (e.g., highly distinguishing signs and symptoms) may arise to identify discrete nosologic classes.
Currently we favor a mixed model
in our project, as do most of the workers in the field. In simplest terms,
we are dealing with the proposition that there is a group of patients less well
put together than neurotic or character-disorder patients, yet not so sick or
disorganized as schizophrenic or other psychotic patients. The basic hypothesis
is that such a group of patients can be defined with clinical criteria, and that
a group so delineated will prove to be different from neurotic and character-disorder
patients on the one hand, and schizophrenic patients on the other, in terms of
manifest psychopathology, past history, course and outcome, pharmacologic responsivity,
and genetic loading. We thus use a continuous model in identifying patients as
borderline, but we then examine the proposition that patients so diagnosed will,
in fact, comprise a discrete nosologic class.
- Hartocollis, Peter, Borderline
Personality Disorders: The Concept, the Syndrome, the Patient, International Universities
Press: New York. 1977.
Update
The Diagnostic and Statistical Manual
of Mental Disorders, Fifth Edition,
Alternative Model Conceptualization
of Borderline Personality Disorder:
A Review of the Evidence
- Vanwoerden, S., & Stepp, S. D. (2022). The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, alternative model conceptualization of borderline personality disorder: A review of the evidence. Personality disorders, 13(4), 402–406.
Personal
Reflection Exercise #6
The preceding section contained information
about the three models for the borderline syndrome. Write three case study examples
regarding how you might use the content of this section in your practice.
Peer-Reviewed Journal Article References:
DeShong, H. L., Grant, D. M., & Mullins-Sweatt, S. N. (2019). Precursors of the emotional cascade model of borderline personality disorder: The role of neuroticism, childhood emotional vulnerability, and parental invalidation. Personality Disorders: Theory, Research, and Treatment, 10(4), 317–329.
Meisner, M. W., Bach, B., Lenzenweger, M. F., Møller, L., Haahr, U. H., Petersen, L. S., Kongerslev, M. T., & Simonsen, E. (2021). Reconceptualization of borderline conditions through the lens of the alternative model of personality disorders. Personality Disorders: Theory, Research, and Treatment.
Selby, E. A., Kondratyuk, S., Lindqvist, J., Fehling, K., & Kranzler, A. (2021). Temporal Bayesian Network modeling approach to evaluating the emotional cascade model of borderline personality disorder. Personality Disorders: Theory, Research, and Treatment, 12(1), 39–50.
QUESTION
12
What are the three models Hartocollis proposes for borderline syndrome? To select and enter your answer go to Test.