MentalHealthCE Login


| Login | ||

Healthcare Training Institute - Quality Education since 1979
CE for Psychologist, Social Worker, Counselor, & MFT!!

Section 23
Cognitive
Model of Panic Attacks
Question 23 | Test | Table of Contents
Ever since Freud's (1894/1940a) classic essay on anxiety neurosis,
it has been accepted that panic attacks are a frequent accompaniment of certain
types of anxiety state. However, it is only relatively recently that panic attacks
have become a focus of research interest in their own right. This shift in emphasis
is largely a result of the work of Donald Klein. In a series of studies which
started in the 1960s, Klein and his colleagues (Klein, 1964; Zitrin, Klein, &
Woerner, 1980; Zitrin, Klein, Woerner & Ross, 1983; Zitrin, Woerner &
Klein, 1981) obtained results which they interpreted as indicating that anxiety
disorders which are characterized by panic attacks respond to imipramine while
anxiety disorders which are not characterized by panic attacks fail to respond
to imipramine. This apparent "pharmacological dissociation" led Klein
(1981) to propose that panic anxiety is qualitatively different from nonpanic
anxiety. This view was endorsed by the writers of the diagnostic and statistical
manual, 3rd Revision (DSM--llI, American Psychiatric Association, 1980) when they
created the two diagnostic categories of panic disorder and agoraphobia with panic,
and used the presence or absence of panic attacks as a major criterion for distinguishing
between different types of anxiety disorder.
Following publication of DSM-II1, there was an enormous increase in research on panic attacks. Perhaps because drug studies were the major stimulus for the creation of the diagnostic category of panic disorder, most recent research has concentrated on biological approaches to the understanding of panic. However, Beck, Emery, and Greenberg, (1985) and Clark (1979, l986a) have argued that panic attacks might be best understood from a cognitive perspective. In this chapter, a cognitive model of panic attacks is described, the extent to which the model is consistent with existing knowledge is discussed, and the initial findings from a series of experiments which are designed to test predictions derived from the model are reported.
Paradoxically, the cognitive model of panic attacks is perhaps most easily introduced by discussing neurochemical and pharmacological approaches to the understanding of panic. A large number of studies have shown that several biochemical and physiological manipulations frequently induce panic attacks in patients who suffer from attacks but rarely induce attacks in nonpanic patients or normal controls. These manipulations include infusions of sodium lactate (Appleby, Klein, Sachar, & Levitt, 1981; Liebowitz et al., 1984), yohimbine (Charney, Heninger, & Breier, 1984), and isoproterenol (Rainey, Pohi et a!., 1984); oral administration of caffeine (Charney, Heninger, & Jatlow, 1985); intravenous administration of caffeine (Uhde, Roy-Byrne, Vittone et al., 1985) voluntary hyperventilation (Clark, Salkovskis, & Chalkley, 1985), and inhalation of carbon dioxide (van den Hout & Griez, 1984). The success of these chemical, physiological, and gaseous manipulations in inducing panic attacks in patients who suffer from attacks has been taken to indicate that certain biochemical changes have a direct panic-inducing effect, and also that panic is a biological disorder. These conclusions have provided a rationale for the further exploration of drug treatments for panic (Chouinard, Annabie, Fontaine, & Solyom, 1982; Zitrin, 1983), and also for studies which attempt to identify neurochemical abnormalities in panic patients (Charney et a!., 1984; Nesse, Cameron, Curtis, McCann, & Huber-Smith, 1984).
However, studies of two of the induction techniques in normal subjects suggest an alternative, psychological explanation for the effectiveness of these diverse manipulations. The first study (Clark & Hemsley, 1982) investigated individual differences in affective response to hyperventilation. A group of normal subjects were asked to hyperventilate in a highly standardized fashion for 2 minutes. Although many subjects became somewhat anxious, considerable individual variation in affective response was observed, with some subjects experiencing hyperventilation as pleasurable. Furthermore, there was some indication that variability in affective response was partly determined by cognitive factors. In particular, subjects' recollection of the context in which they had previously experienced the induced sensations appeared to relate to whether they experienced hyperventilation as pleasant or unpleasant. Subjects who recollected having experienced the sensations during a drug-induced high or during sex experienced hyperventilation as pleasant. Subjects who recollected having experienced the sensations when about to faint or in other unpleasant contexts experienced hyperventilation as aversive.
The
second study (van den Hout & Griez, 1982b) directly investigated the role
of cognitive factors in determining response to the CO2 inhalation technique by
systematically manipulating subjects' expectancy of affective change following
CO2 inhalation. One group of subjects were given the expectation that CO2 would
produce a calm state of relaxation, while another group were told that CO2 would
produce a mildly aversive state. The results were broadly consistent with the
experimenters' hypothesis. Subjects given the expectation that CO2 would produce
a pleasant state did indeed experience a pleasant state, while those who were
given the opposite expectation tended (nonsignificantly) to experience an unpleasant
state. Both of these studies raise the possibility that panic-induction techniques
may not have a direct panic-producing effect but may only provoke panic if the
bodily sensations which they induce are interpreted in a particular way. This
is the central notion behind the cognitive model of panic.
A
COGNITIVE MODEL OF PANIC ATTACKS
In the cognitive model it is proposed
that panic attacks result from the catastrophic misinterpretation of certain bodily
sensations. The sensations which are misinterpreted are mainly those which are
involved in normal anxiety responses (e.g., palpitations, breathlessness and dizziness)
but also include some other sensations. The catastrophic misinterpretation involves
perceiving these sensations as much more dangerous than they really are, and in
particular, interpreting the sensations as indicative of an immediate, impending
disaster. Examples of catastrophic misinterpretations would be a healthy individual
perceiving heart palpitations as evidence of an impending heart attack; perceiving
a slight feeling of breathlessness as evidence of impending respiratory arrest
and consequent death; or perceiving a shaky feeling as evidence of impending loss
of control and insanity.'
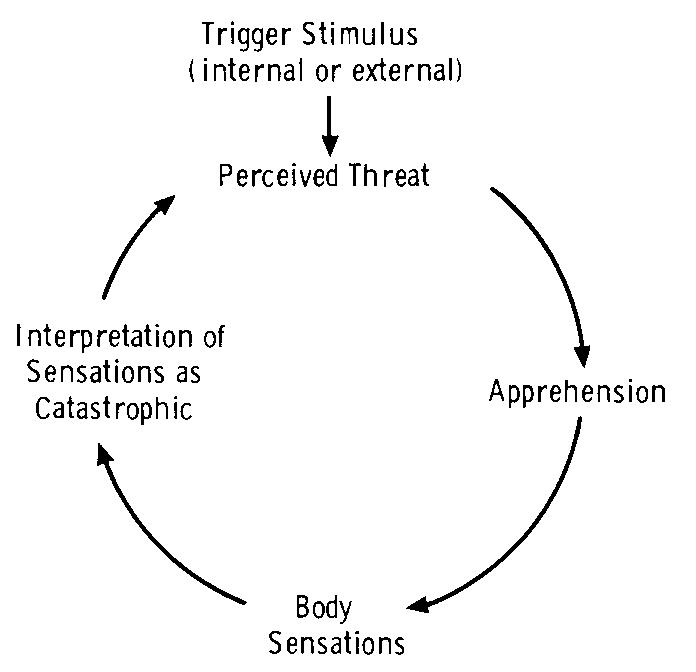
Figure 5.1 illustrates
the sequence of events that is suggested to occur in a panic attack. A wide range
of stimuli appear to provoke attacks. These stimuli can be external (such as a
supermarket for an agoraphobic who has previously had an attack in a supermarket)
but more often are internal (body sensation, thought, or image). If these stimuli
are perceived as a threat, a state of mild apprehension results. This state is
accompanied by a wide range of bodily sensations. If these anxiety-produced sensations
are interpreted in a catastrophic fashion a further increase in apprehension occurs.
This produces a further increase in body sensations and so on, round in a vicious
circle, which culminates in a panic attack.
- Rachman, S. & Jack Maser,
Panic: Psychological Perspectives, LEA Publishers: Hillsdale, 1988.
Personal
Reflection Exercise #11
The preceding section contained information
about the cognitive model of panic attacks. Write three case study examples regarding
how you might use the content of this section in your practice.
Reviewed 2023
Peer-Reviewed Journal Article References:
Fayn, K., Silvia, P. J., Dejonckheere, E., Verdonck, S., & Kuppens, P. (2019). Confused or curious? Openness/intellect predicts more positive interest-confusion relations. Journal of Personality and Social Psychology, 117(5), 1016–1033.
"Reward processing and future life stress: Stress generation pathway to depression": Correction to Mackin et al. (2019) (2019). Journal of Abnormal Psychology, 128(6), 492.
Yang, F., Knobe, J., & Dunham, Y. (2020). Happiness is from the soul: The nature and origins of our happiness concept. Journal of Experimental Psychology: General. Advance online publication.
QUESTION
23
In the Cognitive Model, proposed by Rachman, what is the result of
panic attacks? To select and enter your answer go to Test.