MentalHealthCE Login


| Login | ||

Healthcare Training Institute - Quality Education since 1979
CE for Psychologist, Social Worker, Counselor, & MFT!!

Section 24
Prediction
of Wife Assault
Question 24 | Test | Table of Contents
A woman asks her counselor whether her fiancé is someday likely
to abuse her. He recently told her that his father had beaten him severely as
a child. She also suspects that his abuse of alcohol is more serious than he lets
on.
A judge wonders whether she should sentence an assaultive husband to a treatment program. Several years ago the man was imprisoned for selling drugs, and he made a mockery of the prison's treatment programs.
An intake counselor at a domestic abuse program, asks his supervisor whether a man he is assessing should be treated immediately or wait a month for group treatment. The man has been violent outside the home, including fights with friends and police officers when he was drunk. His wife called to say that she does not feel safe staying at her mother's house. He once came through a window there and knocked her mother down in his attempt to find her.
These are just some of the types of situations practitioners routinely face that call for the prediction of domestic violence. Although the science of predicting wife assault is quite inexact, practitioners frequently make informal risk assessments of future violence (Gottfredson & Gottfredson, 1988). In some situations they are legally mandated to assess imminent danger and to attempt to avert a tragedy. As domestic abuse programs work more closely with criminal justice agencies, their staff increasingly will be asked to make formal predictions. Thus, although the "state of science" in this area is imprecise, practitioners need the best information available.
The purpose of this chapter is to provide the latest scientific information on risk factors for wife assault and the clinical assessment of these factors. Special attention is given to predicting serious assault because of its severe consequences, including the possibility of homicide. Other types of prediction also are covered: What factors are related to recidivism after abuser treatment? When child custody is decided, is the abuser or his partner at more risk for abusing the children? What are the odds that a man who batters will be violent in a new relationship? Prediction in this area has many important applications-in sentencing, probation work, and treatment. Examples of these applications are given.
When the terms wife and marital are used, unless otherwise noted they refer to cohabiting relationships as well. Major studies of risk factors combined cohabiting and married cases. Risk factor research on dating violence is less well developed and has been reviewed elsewhere (Sugarman & Hotaling, 1991).
Review of
Risk Markers
A review of risk markers is given for various types
of domestic assault. We cannot say for certain whether a risk marker is a causal
predictor. The first step in developing a predictive model is often the uncovering
of factors associated with a phenomenon (Mercy & O'Carroll, 1988). These markers
may simply co-occur with the abuse. Or they may precede the abuse, but only because
they are related to a true causal factor. Longitudinal studies provide stronger
evidence of causal connections, but these studies are rare in the field of domestic
violence. Therefore, care is taken in this review to primarily use the terms risk
marker or risk factor instead of predictor. From a practical standpoint, however,
risk markers still may be useful in alerting practitioners when to expect violence
or what type to expect.
The science of predicting violence may never be very good, especially for violence that is infrequent. This non-precision is simply a matter of the difficulty in predicting rare events. The problem we face is that serious forms of violence are generally the least frequent. Homicide, for example, is the most difficult to predict because it is rare, compared with other violence, yet it is the behavior that is likely to concern us most (see Sherman, 1992, for discussion). This review begins with the more common forms of domestic violence before turning to its severe forms.
RISK
FACTORS FOR ASSAULT
Our knowledge of what distinguishes assaultive
from nonassaultive men has grown steadily in the past decade. Recent reviews of
the empirical literature document the existence of a number of risk factors that
are found consistently across studies (Hotaling & Sugar-man, 1986; Tolman
& Bennett, 1990). The findings, however, should not obscure the possibility
that men who batter may not be too different from other men. Men, who batter,
may be at one end of a continuum of male socialization.
Risk factors that are found most consistently are presented first, followed by those showing less consistency. No attempt is made to place these factors into a detailed theoretical framework.
Violence in Family of Origin: As one might expect, men who batter experienced family violence in their childhoods. There may be a somewhat stronger effect for witnessing violence than for being its target (Hotaling & Sugarman, 1986). Even so called minor violence or punishment against boys is a risk factor for them becoming domestically assaultive (Straus, 1980). Men who both witnessed violence and suffered directly from it are even more likely to be domestically violent. Social learning theory may provide the most parsimonious explanation for this intergenerational transmission, but it is not the only plausible explanation.
Demographic Factors: Although wife assault cuts across all socioeconomic groups, it is more prevalent among men with lower in-comes and less education (Hotaling & Sugarman, 1986). Differences between the demographics of the partners also appear to place the men at risk. For example, differing religious backgrounds was a risk marker in all three studies that investigated this factor (Hotaling & Sugarman, 1986). The woman's greater education or occupational status was a risk factor in most studies, possibly because her status threatened the patriarchal beliefs of the man. This was not as prominent a risk factor as other demographics, but it is one that is extremely easy for the practitioner to uncover.
Alcohol: High rates of alcohol use or alcoholism appear characteristic of most abusers. Tohnan and Bennett (1990) calculated the percentage of chronic alcohol abusers or alcoholics across 13 studies of batterers to be nearly 60% (median). Intoxication at the time of the violence is less clearly a risk marker. Coleman and Straus's (1983) findings suggest that severe intoxication may decrease violence.
Behavioral
Deficits: Several researchers have found that men who batter report being
less assertive than other men (Douglas, Alley, Daston, Svaldi-Farr, & Samson,
1984; Maiuro, Calm, & Vitaliano, 1986; Rosenbaum & O'Leary, 1981). In
one study the men were assertive in saying no to requests but were not adept at
"initiating" forms of assertiveness (Maiuro et al., 1986). Dutton and
Strachan (1987) found that low verbal assertion was related to violence in men
with the greatest need for power. This need probably produced greater anger and
anxiety in them, and violence erupted when they did not have the skills to handle
their feelings. Margolin and her associates (Margolin, John, & Gleberman,
1988) observed couples interact and found some behavioral excesses by violent
husbands:
They had more negative voice qualities and more signs of irritation
and frustration.
Psychopathology: The magnitude
of the problem of woman abuse and the evidence for socio-cultural factors has
minimized attention to psychopathology. Although only a small percentage of abusers
appear to have severe mental disorders, broad definitions of psychopathology may
be applicable to most abusers (e.g., Axis II disorders). Most abusers in treatment
programs show clinical elevations on at least some of the subscales of the Millon
Clinical Multiaxial Inventory (MCMI) (Millon, 1983) and the Minnesota Multiphasic
Personality Inventory (MMPI) (Coates, Leong, & Lindsey, 1987; Hamberger &
Hastings, 1986). Profiles of psychological tests match clinical impressions of
the men (Bernard & Bernard, 1984; Schuerger & Reigle, 1988). One average
MMPI profile described the abuser as distrustful of others, isolated, and feeling
insecure and alienated. The men maintain a strong masculine identification although
they may be excessively concerned about their own masculinity (Bernard & Bernard,
1984). No consistent profile has been found on the MCMI (Hamberger & Hastings,
1986). Pathology may be related to alcoholism because one study found that alcoholic
batterers were most likely to have clinical elevations on the MCMI (Hamberger
& Hastings, 1991). Chronic alcohol abuse,
for example, could lead to paranoia.
Surveys show that about half of the men who batter their wives also batter their
children.
Violence Toward Children: Both random and nonrandom surveys consistently show that about half of the men who batter their wives also batter their children (Saunders, 1994). Most studies defined violence toward the children as more severe than a slap or a spanking. In the random survey by Straus (1983), 50% of the violent husbands and 7% of the nonviolent husbands abused their children.
Battered women are also above normal risk for abusing their children, but it is much lower than the risk that the men will do so. The women's violence seems to be situationally related, whereas the men's abuse of the children seems related to chronic problems such as alcohol abuse amid their own childhood traumas (Saunders, 1994).
Anger: Anger and hostility are not consistently related to violence. The type of measure may explain this inconsistency. The Buss-Durkee Hostility Inventory (Buss & Durkee, 1957) and responses to videotapes of women "engulfing" or "abandoning" their partners reveal anger in domestic assaulters. Their anger does not necessarily exceed that of nondomestic assaulters (reviewed in Tohnan & Bennett, 1990). When anger is measured on the Novaco Anger Index (Novaco, 1975), a measure of situations likely to evoke anger, men who batter do not score above the norm. When this index is modified to be maritially specific, it is related to aggressive behavior reported by the women (Saunders & Hanusa, 1986). Thus the type of situation makes a difference, consistent with the feminist view that women are the targets of men's displaced anger or that anger erupts when women break the rules of patriarchy.
Stress: Like anger, stress does not appear to be consistently related to violence (Hotaling & Sugarman, 1986). Some evidence suggests that men's work stress is a risk factor (Baring & Rosenbaum, 1986). Studies that show a link between "external stress" and violence (e.g., Straus, 1980) are difficult to interpret because many of the items may be the result, rather than the cause, of violence. For example, items like "divorce," "separation," and "problems with the boss" are likely to be the direct result of aggressive behavior, and not their cause.
Depression and Low Self-Esteem: The causal role of depression is also difficult to decipher. Men who batter generally appear to score above the norm on standard measures of depression (Tolman & Bennett, 1990) and in one study were more depressed than nondomestic assaulters (Maiuro et al., 1986). However, their depression may be the result of the arrest and separation that often precede treatment. Some evidence shows that batterers who are not publicly detected are not depressed (Hamberger & Hastings, 1990).
Although related to depression, self-esteem may not respond to situational losses and stress as much as measures of depression. Three of the five studies reviewed by Hotaling and Sugarman (1986) showed that men who batter suffered from low self-esteem.
Non-risk Factors: Researchers have been surprised to find that traditional sex role attitudes have not distinguished batterers from non-batterers. At least six studies have had non significant results (Hotaling & Sugarman, 1986). One explanation is that only some types of batterers have traditional attitudes. Evidence for this explanation is presented later.
The majority of studies also have not found evidence that these men have greater decision-making power in the relationship or a need for power. The largest and most representative study, however, does show power imbalance to be a risk marker (Straus, Gelles, & Steinmetz, 1980). The factor may be important also for only a subset of abusers; for example, one study found it to be a factor for blue-collar men with few "resources" (Allen & Straus, 1980). Another study found that men's perceived powerlessness was associated with violence (Babcock, Waltz, Jacobson, & Gottman, 1993). Cross-cultural studies clearly indicate patriarchal norms and sexual inequality as risk factors (Levinson, 1989; Yllö, 1983).
Concomitants: Some factors may be seen frequently in conjunction with abuse but are probably concomitants, rather than useful risk factors. For example, marital distress and arguments and conflict in the relationship are often associated with violent relationships (O'Leary & Vivian, 1990; Straus et al., 1980). Sexual assault often co-occurs with physical abuse as well (Hotaling & Sugarman, 1986).
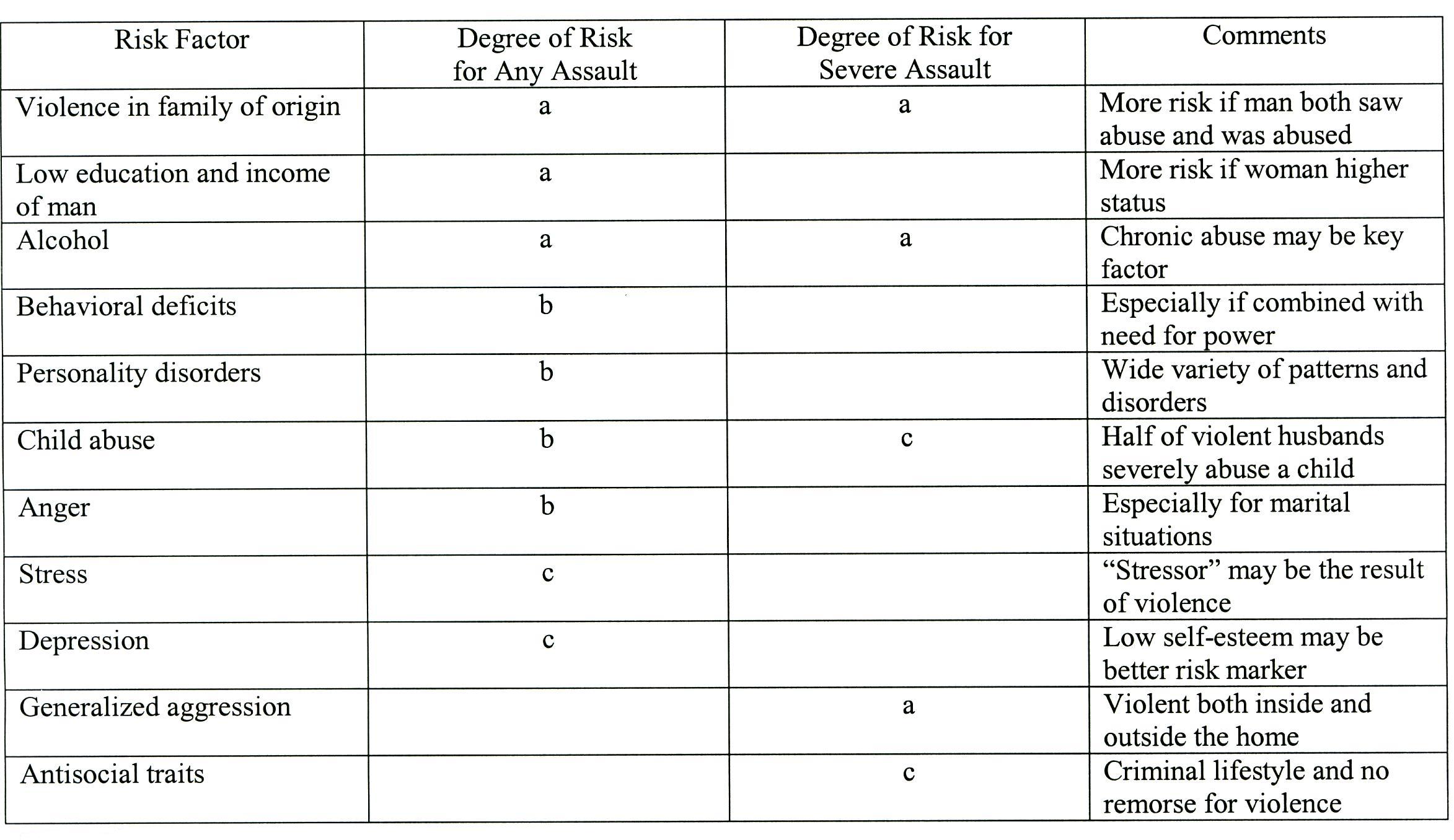
a
= prominent risk; b = probable risk; c = possible risk
Summary:
This Table lists the risk factors described above and labels them as "prominent,"
"probable," or "possible," according to the strength of evidence
supporting them. The table also lists characteristics of the severe assaulter,
to be described later. Many of the studies reviewed used samples of men in treatment,
and thus the findings may not apply to other men)
- Campbell, J. C., PhD. (1997). Assessing Dangerousness. London, England: Sage Publications, Inc
Peer-Reviewed Journal Article References:
Chen, J., Walters, M. L., Gilbert, L. K., & Patel, N. (2020). Sexual violence, stalking, and intimate partner violence by sexual orientation, United States. Psychology of Violence, 10(1), 110–119.
Crossman, K. A., & Hardesty, J. L. (2018). Placing coercive control at the center: What are the processes of coercive control and what makes control coercive? Psychology of Violence, 8(2), 196–206.
Dichter, M. E., Thomas, K. A., Crits-Christoph, P., Ogden, S. N., & Rhodes, K. V. (2018). Coercive control in intimate partner violence: Relationship with women’s experience of violence, use of violence, and danger. Psychology of Violence, 8(5), 596–604.
QUESTION
24
Male batterers score above the
norm on standardized measures of depression. However, male
batterers were more depressed than what group? To select and enter your answer go to Test.