MentalHealthCE Login


| Login | ||

Healthcare Training Institute - Quality Education since 1979
CE for Psychologist, Social Worker, Counselor, & MFT!!

Section 11
BPD and Interpersonal Relations
Question
11 | Test
| Table of Contents
The survey of a wide variety of psychotic symptoms reveals that
the borderlines do not have any continuous or severe psychotic experiences. Some
of the borderlines report possible hallucinatory experiences of both auditory
and visual types. These are unrelated to drug usage and prove difficult to evaluate
clinically. Most commonly the borderlines report psychotic ideation in the depressed
area- namely, extended periods of feeling worthless or hopeless. It is rare to
find a more outright delusional depressive percept such as the belief of having
hurt someone or committed a crime. The only other psychotic symptom reported with
frequency is ideas of reference. Many patients have had periods when they felt
unduly suspicious of others' intentions. They characteristically feel uncertain
or uncomfortable about any psychotic experience. The interviewers generally noted
that the psychotic percept is at least not bizarre and totally unfeasible. There
are virtually no nihilistic or religious delusions, delusions of thought-insertion,
interference, or broadcasting, or delusions of somatic passivity. Many borderline
patients had been hospitalized or treated in individual psychotherapy. As predicted,
they often report that these experiences made them worse. Contrary to expectations,
these patients rarely experience severe or continuous dissociative experiences
of any kind. Depersonalization experiences are somewhat more likely than derealization.
The least common dissociative experience is feeling things are changing size or
shape and the most common is feeling physically separated from one's feelings.
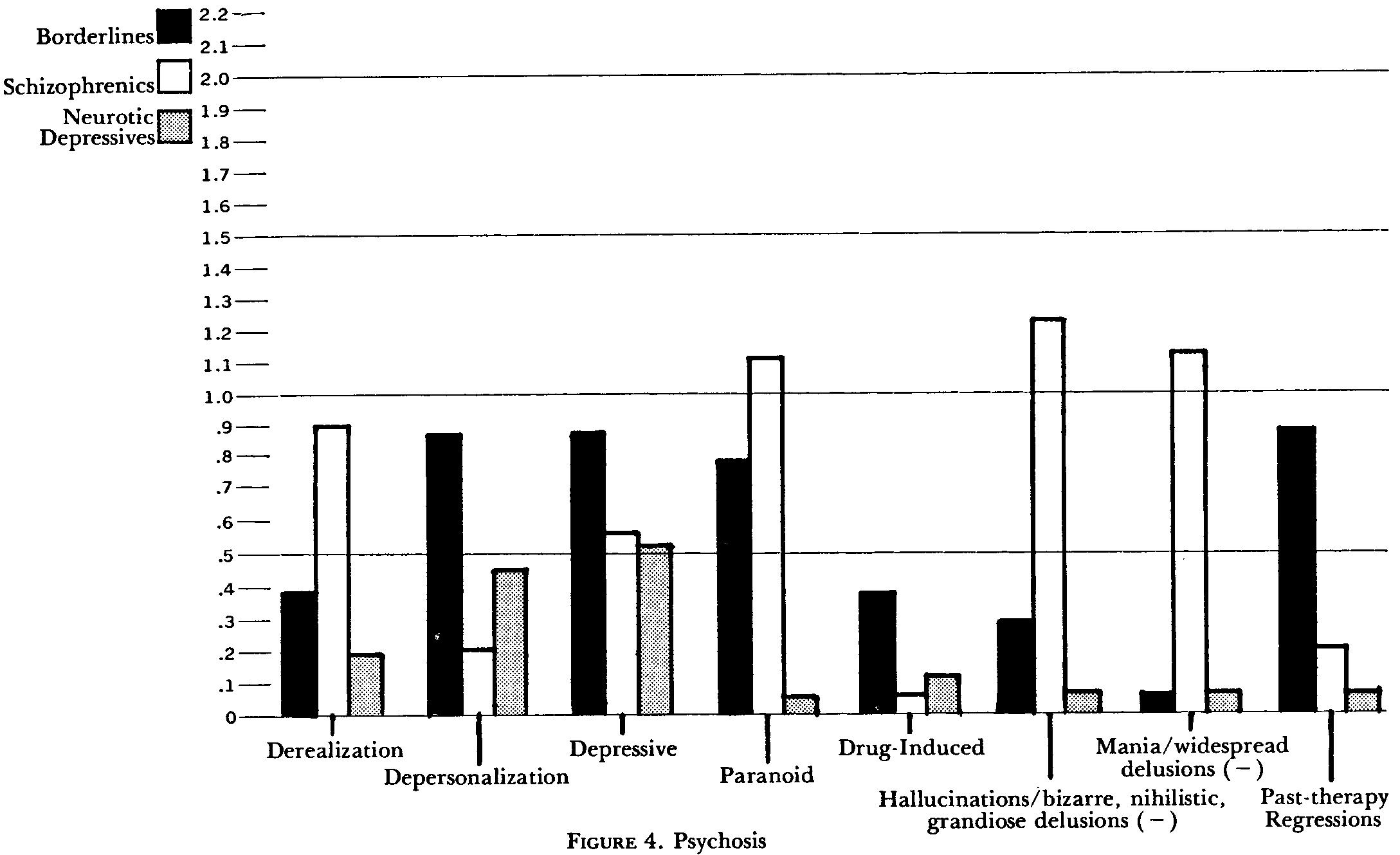
Figure 4 shows that, in addition to their surprisingly low frequency, derealization experiences actually discriminate the schizophrenics, who experience them more frequently (p .023). No significant differences are apparent for depersonalization. Nor does any difference appear for psychotic depressive symptoms. The borderline sample has more brief paranoid experiences than the neurotic group (p = .014) but not than the schizophrenics. The latter group, however, is much more likely to have widespread delusional beliefs in other areas (Ji <.001), which makes clinical discrimination quite easy. Although borderlines are slightly more likely to report psychotic experiences from marijuana or alcohol or persisting psychotic symptoms after psychotomimetics, this occurs too infrequently in these samples for any significant differences to surface. As expected, the schizophrenic sample presents significantly more of those psychotic symptoms specifically felt to be unlikely in borderlines, i.e., hallucinations, nihilistic and grandiose delusions, and patently absurd or bizarre delusional content (~ <.001). In hearing about past psychiatric contacts, the interviewers judged that the borderlines develop transient psychotic experiences within psychotherapy or have had a behavioral regression after hospitalization with much more frequency than either the schizophrenics (p = .003) or the neurotic depressives (p = .004). The section total score is significantly higher for the borderlines than for the neurotics (p = .012) but not than for the schizophrenics.
INTERPERSONAL RELATIONS
Borderlines associate with many people and spend most of their time in the presence
of others. They feel a need to have people around and report being bothered when
alone. They consider that they have close friends and manage to keep in touch
with these people. Almost all of them tend to feel sorry for and make efforts
to take care of others. Yet they decidedly do not like having others take care
of them and find this uncomfortable when it occurs. This apparent paradox continues
in their commonly describing having someone in their lives whom they feel they
need but less often having someone who they feel needs them. They usually find
it uncomfortable to live with their families of origin and yet they often long
to be with their parents when they are away from home.
Their most intense current relationships are frequently troubled by breakups. Their relationships are strongly dependent, masochistic, and marked by devaluation and conscious manipulative efforts. The interviewers could frequently see similarities between these interactional patterns and those described in the patient's relation to one of his parents -usually the mother. The current interactions seem to serve a substitutive function.
During the research interviews, the borderlines are often quite suspicious and problems in rapport are common. Their past psychiatric hospitalizations often include a history of presenting special problems for the staff.
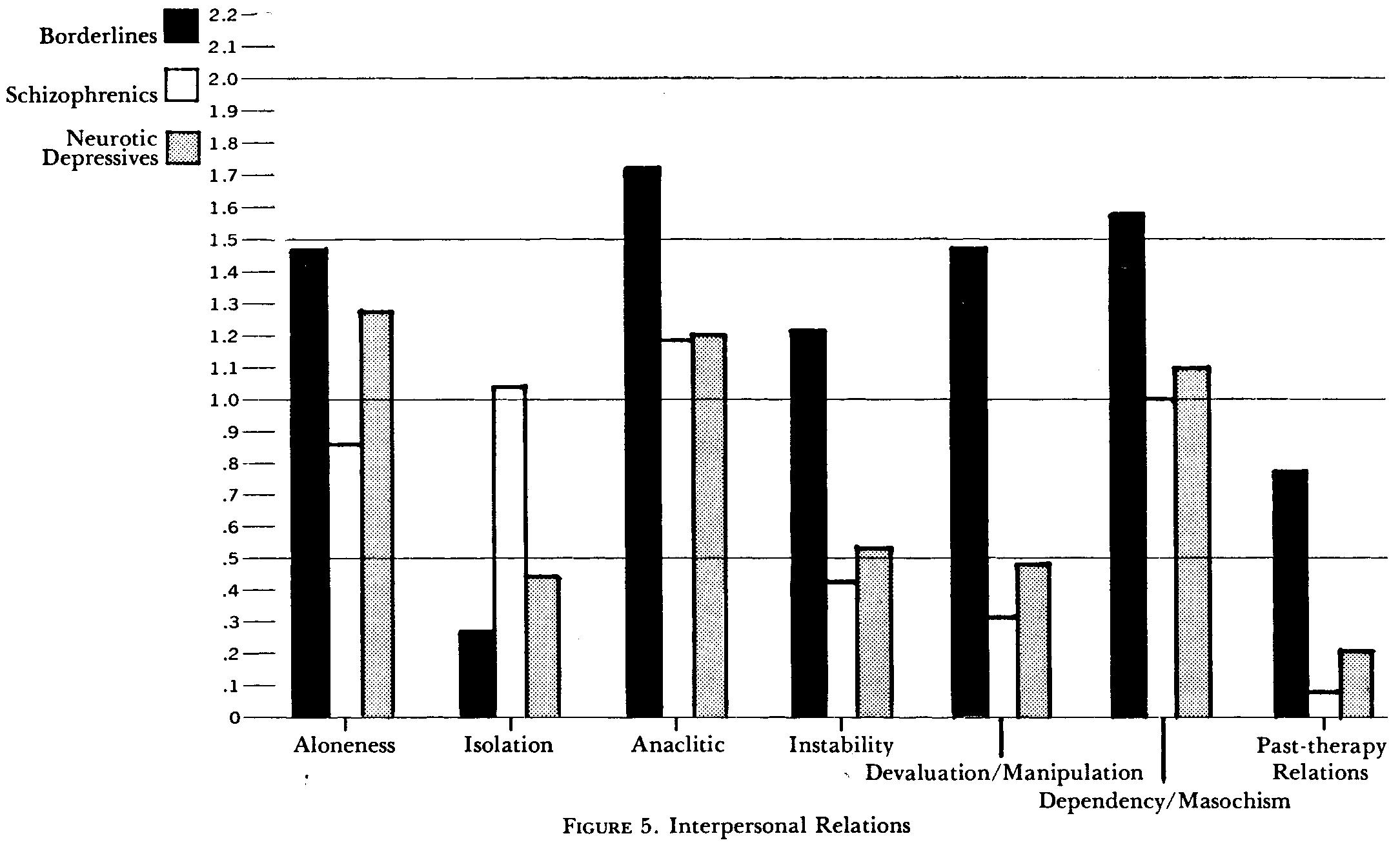
The
summary statements all discriminate between one or both groups in this section
(see Figure 5). The borderlines differ from schizophrenics both in their disinclination
to and their difficulty in being alone (p = .0 1). The schizophrenics are more
often judged to be socially isolated "loners" (p <.001). The borderlines
seek anaclitic relations in which they act as care givers, yet they are in active
conflict about giving and receiving care. These patterns are less common for both
the scbizophrenics (p = .006) and the neurotics (p = .029). The quality of borderlines'
close relationships are more intense and unstable than for either the schizophrenic
(p = .001) or neurotic sample (p = .02). Problems with devaluation, manipulation,
and hostility are so characteristic and discriminatory that they contrast with
both comparison groups (p <.001). Problems with dependency and masochism are
also highly characteristic but only differ significantly from the schizophrenic
sample (p .006). After reviewing past relations with therapy persons, the interviewers
concluded that the borderline patients have almost always been involved in some
problem with staff splitting, countertransference problems, or "special"
relations to their past therapist (p <.001 with the schizophrenics, p = .005
with the neurotic depressives). This section is highly discriminatory over-all
between borderlines and both schizophrenics (p <.001) and neurotics (p= .005).
- Hartocollis, Peter, Borderline Personality Disorders: The Concept, the Syndrome,
the Patient, International Universities Press: New York. 1977.
Update
Momentary Interpersonal Processes
of Suicidal Surges
in Borderline Personality Disorder
- Kaurin, A., Dombrovski, A. Y., Hallquist, M. N., & Wright, A. G. C. (2022). Momentary interpersonal processes of suicidal surges in borderline personality disorder. Psychological medicine, 52(13), 2702–2712.
Personal
Reflection Exercise #5
The preceding section contained information
about BPD psychosis and interpersonal relations. Write three case study examples
regarding how you might use the content of this section in your practice.
Peer-Reviewed Journal Article References:
De Panfilis, C., Schito, G., Generali, I., Gozzi, L. A., Ossola, P., Marchesi, C., & Grecucci, A. (2019). Emotions at the border: Increased punishment behavior during fair interpersonal exchanges in borderline personality disorder. Journal of Abnormal Psychology, 128(2), 162–172.
Haliczer, L. A., Woods, S. E., & Dixon-Gordon, K. L. (2021). Emotion regulation difficulties and interpersonal conflict in borderline personality disorder. Personality Disorders: Theory, Research, and Treatment, 12(4), 347–353.
Howard, K. P., Lazarus, S. A., & Cheavens, J. S. (2021). A longitudinal examination of the reciprocal relationship between borderline personality features and interpersonal relationship quality. Personality Disorders: Theory, Research, and Treatment.
QUESTION
11
How do borderlines differ from schizophrenics? To select and enter your answer go to Test.